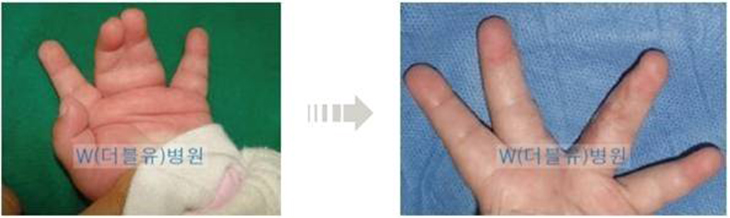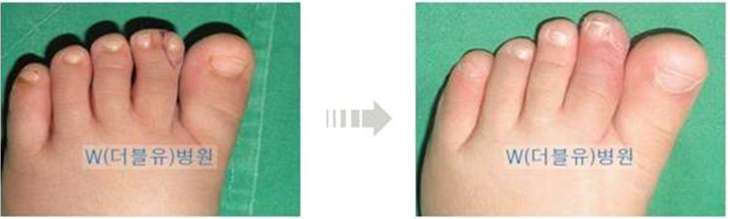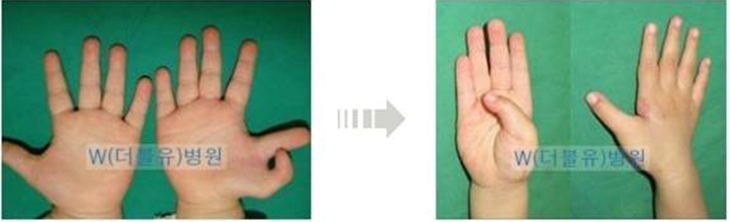
Polydactyly refers to the condition of more than6 fingers or toes. The most frequent symptom is the formation of another finger on the thumb or the little finger.
In the case of the Polydactyly of the thumb, the extent and the range of the surgery differ very much due to extensive range of configuration, arrangement and sizes of the bones, ligament and tissues.
In the case of the Polydactyly that occurs on the thumb, past family history accounts for only 10% of the cases and it is deemed to occur sporadically.
Therefore, it is deemed that there need not be serious concerns for the genetic cause of Polydactyly.
In simple cases in which only the tissues are attached, surgical procedure can be performed easily. However,
if bones, joints and ligaments are connected complexly, it becomes a difficult and complicated surgical
procedure that requires several surgical procedures to achieve normal appearances and functions of the fingers.
Therefore, efforts need to be put in to prevent such malformation at the time of the first surgery.
- 1. Time of the surgery
- In the modern medicine, it is the widely accepted theory that it is advisable to perform surgery on congenital malformation as early as possible. Moreover, parents wish to illustrate normal hands of the infant to the relatives and friends at the 100-day or 1st birthday party. Accordingly, they request the surgery be performed prior to the 100th day of the birth of the infant. In the case of simple Polydactyly, it is possible to perform the surgery prior to the 100th day of the birth. However, if the problems of the bones, joints and ligaments are accompanied, it is advisable to perform the surgery at around 1 year from the birth. Accordingly, there is a trend of undergoing primary surgery at about 8~10 months after birth nowadays.
- 2. Anesthesia and surgical technique
-
In simple cases, it is possible to perform excision simple sedation anesthesia. The condition of the infant prior to the surgery becomes more important earlier the surgery is performed. It is advisable to postpone the surgery by about 2 weeks if there are symptoms of common cold in the infant. Sedation anesthesia, unlike the general anesthesia, refers to the performing the surgery by injecting localized anesthesia in the hand while the infant is in sedated conscious state. When the infant is fully awake after the surgery, the infant can be taken home immediately. However, in the case of the surgery that takes long time with the need to work on the joints, ligaments and bones, general anesthesia is necessary along with 1~2 days of hospitalization.
The surgical techniques can be categorized largely into the following simple excision procedure, reconstruction procedure following excision and Bilhaut-Cloquet procedure.
- A. Simple excision procedure
- If only the tissues are attached, it is possible to remove the unnecessary tissues by using string or devices immediately after the birth. However, if bone structure is involved, it is possible to perform excision surgery at about 5~6 months after birth at which sedation anesthesia can be implemented.
- B. Reconstruction procedure following excision
- In general, if the fingernail size of the polydactyly finger becomes 70~80% of that of the normal finger, the remaining finger is excised. At this time, excision is made by ensuring that the necessary tissues are preserved rather than simply cutting off the excess finger because it is necessary to improve the appearance and function of the finger by suturing the tissues of the surplus finger to be excised with the tissues of the finger left intact if the bones, joints and ligaments are interconnected. In majority of the cases, the joint needs to be reconstructed since the ligaments that form the joints of the finger are weak. Rarely, osteotomy of portion of the bone is necessary as well.
- C. Bilhaut-Cloquet procedure
- If 2 polydactyly fingers have similar size and neither has fingernail size that is 70% of that on normal finger at the maximum, surgical technique of combining the 2 fingers to create a single finger is performed. After having appropriately cut the bones and joints of the both fingers, bones are fixated and the ligaments are connected. However, in this case, 2 fingernails are combined to make one fingernail, there is the problem of the split in the fingernail as it grows and the reconstructed joint would have deteriorated functions.
- 3. Complications: Secondary corrective procedure
-
Simple complication that is observed commonly after the primary surgery include bulging of portion of the bone with the regrowth of the bone due to the failure to completely remove the growth point of the bone in the excised finger. In such case, it is possible to make correction by excising the bone and the surrounding tissues that are bulging out.
However, in the case of polydactyly thumb, it grows in Y-shape from birth and will not grow in straight line even if one of the axes is cut off. Just as one of the axes of Y is cut off, the remaining portion does not become straight, the formation of deformation due to the bending of the joint after the primary surgery is referred to as the 'Z' shaped deformation of the finger (angle formation).
Although the extent of the results following the surgery in the case of Polydactyly with complicated configuration differs substantially, it is the most common complication that does not fail to manifest. Accordingly, it would not be excessive to emphasize the importance of the primary surgery repeatedly for this reason. Therefore, maximum efforts need to be put in to prevent this deformation at the time of the primary surgery. Although it differs amongst various scholars, a surgical procedure can be performed at about the age of 5~6 years old if the deformation is severe or corrective surgery is performed by implementing osteotomy at the time of completion of the growth of the bones, that is, at about the time of graduation from elementary school. It is not easy to obtain fully satisfactory results from a single execution of such surgical procedure.
- 4. Care after the surgery
-
In most cases, the suture threads are removed after about 2 weeks, and the area of the surgery can be washed with water thereafter and it is advisable to frequently massage the affected area by using ointment that minimizes formation of scars. In the event of having performed replantating of the ligament for joint reconstruction, it would be advisable to apply cast for about 4 weeks. In addition, it is possible to assist proper growth of the thumb by applying small splint to the hand occasionally in order to prevent secondary Z-deformation.
In conclusion, since the thumb is an important finger that accounts for more than 50% of the functions of the hand, efforts must be put into maintain the anatomical configuration and functions of the thumb as close to the normal condition as possible if there is congenital malformation. For this purpose, the parents need to ponder over when and how to apply surgery from the position of the infant rather than themselves, and the surgeon needs to put utmost efforts in fully reconstructing the functions of the hand without considering it as a simple surgery of excising the surplus tissues.